
Introduction
Main Reference text: Clinically Oriented Anatomy 7th ed, K. Moore.
Erik Korzen DC, NASM CES
Guest Contributor
------------------------
Welcome to the first post of the series related to clinical anatomy. Throughout this series we will be reviewing anatomical structures as well as their clinical significance. Since this is the first of the series, I wanted to provide a foundation for the future posts that will focus on more specific regions of the human body. Generally, this series will concentrate on regional anatomy as opposed to systemic anatomy which will allow us to integrate biomechanics and physiology into the anatomy being presented.
The significance of clinical anatomy is that it differs from strictly rote memorization of anatomical structures. For example, as opposed to asking “What is the origin of the long head of the biceps femoris muscle?”, clinical information would require us to ask “Where would an avulsion tear of the long head of the biceps femurs muscle be located?” In healthcare, a high-level of knowledge in anatomy and physiology is required to solve clinical problems. We hope that this human anatomy series will review already known topics and shed light on less clear ones.
Let’s get back to the basics of human anatomy!
Anatomical Terms
Anatomical position (our reference for everything in anatomy)
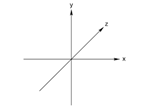
4 Imaginary planes:
Median (Sagittal or Mid-Sagittal)
Frontal (Coronal)
Transverse
Oblique (combo of multiple planes)
Relate these 3 imaginary planes to the XYZ axis (that we all probably learned in grade school) and use your own hand to represent each axis. Now you should be able to visualize the rotation around each axis as the basis for describing human movement (a topic we will discuss in future posts).

Terms of Relationship
How do we describe structure A relative to structure B? We need a set of terms to define and compare various structures throughout the body.
• Superior = nearer the head/vertex (cephalad or cranial)
• Inferior = nearer the sole of foot (caudal)
• Anterior = front surface (ventral)
• Posterior = back surface (dorsal)
• Medial = nearer median plane
• Lateral = further from medial plane
• Proximal = nearer the center of the body/core
• Distal = further from the center of the body/core
• Superficial = nearer the surface of the body
• Deep = further from surface of the body
• Rostral = nearer anterior portion of head (commonly used in neuroanatomy)
Laterality Terms
Bilateral = paired structures
Unilateral = structure located on either Right or Left of body
Ipsilateral = structures located on the same side of the body
Contralateral = structures located on the opposite side of the body
Movement Terms
We typically reference the anatomical position as the starting position for movements which occur around the XYZ axis or in the planes.
• Flexion = decreasing angle between bones or parts of body
• Extension = increasing angle
• Dorsiflexion = flexion at ankle joint (toes towards the nose)
• Plantarflexion = flexion at ankle joint (pushing on the gas pedal)
• Abduction = movement away from midline or median plane (EXCEPTION: movement of the digits)
- digits in the foot Abduct/Adduct relative to the 2nd digit
- digits in the hand Abdduct/Adduct relative to the 3rd digit
• Adduction = movement towards midline or median plane (EXCEPTION: movement of the digits)



- digits in the foot Abduct/Adduct relative to the 2nd digit
- digits in the hand Abdduct/Adduct relative to the 3rd digit
• Medial/Internal Rotation = anterior surface moves closer towards midline or median plane
• Lateral/External Rotation = anterior surface moves further from midline or median plane
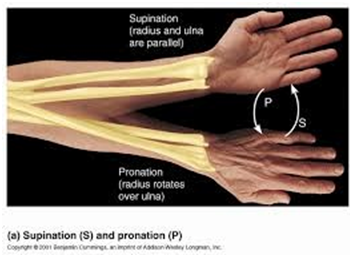
• Pronation = rotation involving palmar surface of hand (or plantar surface of foot) facing more posteriorly
• Supination = rotation involving palmar surface of hand (or plantar surface of foot) facing more anteriorly
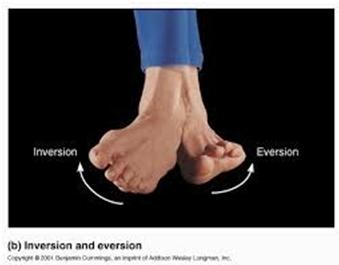
• Eversion = plantar surface of foot moves away from midline or median plane
• Inversion = plantar surface of foot moves towards midline or median plane
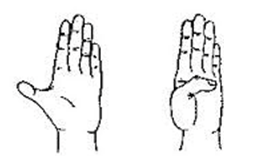
• Opposition = pad of 1st digit in hand (thumb) moves towards another digit
• Reposition = movement of pad of 1st digit in hand (thumb) to anatomical positionEF38E6
• Protrusion/Protraction = anterior movement (scapula or mandible)
• Retrusion/Retraction = movement posteriorly (scapula or mandible)
• Elevation = movement superiorly
• Depression = movement inferiorly
• Circumduction = combination of flexion, abduction, extension, adduction (distal end of extremity moves in circular motion)
So there it is, the foundation for our future human anatomy series. We are “all on the same page” when it comes to reference points, movements and structure description. The incorporation of functional anatomy, biomechanics and even some physiology will be the focus of future posts on specific anatomical regions. As this is intended for healthcare professionals of all variations, musculoskeletal structures will NOT be the only anatomic structures found throughout these posts. I will vehemently attempt to include neurologic, vascular and visceral structures into these reviews.
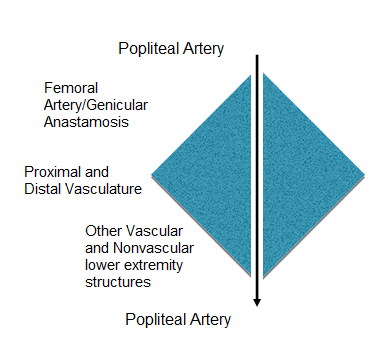
From a more general point of view, I want readers to start thinking in a sort of diamond shaped process. I know that sounds very strange initially but bear with me. I would have used a funnel, but that’s really not how everyday clinical problems are conceptualized. As we think of clinical care, beginning usually with a specific sign or symptom then broadening into the subjective and objective information which leads to a broad list of differential diagnoses (DDx), narrowing into the arena of triage/red flags/indication or contraindications for treatment and finally again narrowing into the diagnosis (Dx) and eventually into specific treatments or request for further diagnostic tests. Anatomy is the SAME.
As we think of studying human anatomy, begin with a specific structure you are interested in then broaden into the regional anatomy and entire human body and finally again narrow into the specific structure. It is important to think this way in order to fully integrate and comprehend the simplicity and intricacy of the human body. It is truly amazing!
Please feel free to connect with the author, Erik Korzen DC, if you have any questions regarding this material. Below is a brief bio for your reference.
Erik Korzen, DC, NASM CES (chiropractic physician/educator)

Dr. Korzen specializes in physical medicine and pain management through conservative care. He owns an evidence-based practice in IL and functions as adjunct faculty for undergrad courses in human anatomy and physiology. He has presented research at a national chiropractic conference and had an article published in ACA News monthly magazine. Dr. Korzen also has his own blog and writes for the Brookbush Institute.
Feel free to check out Dr. Korzen's LinkedIn profile for more info. https://www.linkedin.com/pub/erik-korzen-dc/6a/58a/6b1